
- LVEF ≥50% without regional wall motion abnormalities
- No or mildly dilated LV cavitya without leaflet tethering
- Mitral annulus dilatation (AP >35 mm)
- Enlarged LA (LAVI >34 mL/m2)
Taking the path to treatment together
With transcatheter edge-to-edge repair (TEER), the mitral valve can be repaired. Yet it’s general cardiologists that make it happen.
By identifying the disease and referring your patients to a Heart Team, you can help them move toward the treatment decision that is right for them.

I breathed like an old man. I went to see a lung specialist, who examined me and then straight away sent me to see a cardiologist.
-Reinhold, MR patient
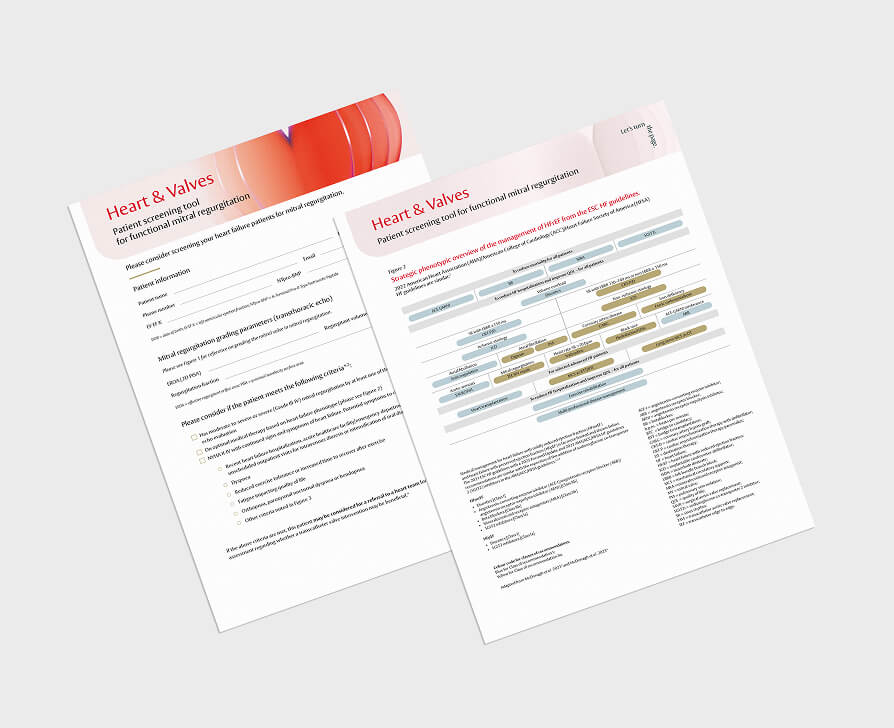
If MR is suspected, echocardiography is the first choice of imaging technique to quantify MR severity, assess the status of the left ventricle and identify MR aetiology as primary (PMR) or secondary (SMR).3,4
Transthoracic echocardiography is commonly used to assess MR, but evaluating its severity is complex. A comprehensive approach is advised, using a mix of quantitative measures and qualitative indicators.5
When you suspect MR in your patient, refer them to a Heart Team for evaluation.4
Use our patient screening tool to help you decide whether you should refer your patient with SMR to the Heart Team for further assessment.

A Heart Team’s multidisciplinary approach means that your patients will receive a thorough evaluation and a personalised treatment plan.6
The 2025 ESC/EACTS recommendations on indications for intervention in severe PMR4

aPlease refer to Table S2 of the ESC/EACTS Guidelines Supplementary data.4
AF: atrial fibrillation; EACTS: European Association for Cardio-Thoracic Surgery; ESC: European Society of Cardiology; LA: left atrium/left atrial; LAVI: left atrial volume index; LV: left ventricle/ventricular; LVEF: left ventricular ejection fraction; LVESD: left ventricular end-systolic diameter; LVESDi: left ventricular end-systolic diameter indexed to body surface area; MV: mitral valve; SPAP: systolic pulmonary artery pressure; TEER: transcatheter edge-to-edge repair; TMVI: transcatheter mitral valve implantation; TR: tricuspid regurgitation.
SMR can be classified as atrial or ventricular depending on certain characteristics. The key criteria for diagnosing atrial and ventricular SMR outlined in the 2025 ESC/EACTS guidelines are presented in the table below.4

aLV end-diastolic dimension of <56 mm in females and <63 mm in males; indexed LV end-diastolic volume <71 mL/m2 (in women) or <79 mL/m2 (in men). AP: anteroposterior; LA: left atrium/atrial; LAVI: left atrial volume index; LV: left ventricle/ventricular; LVEF: left ventricular ejection fraction; SMR: secondary mitral regurgitation.
The 2025 ESC/EACTS recommendations on indications for mitral valve intervention in severe, symptomatic SMR without concomitant coronary artery disease4

aCriteria predicting outcome improvement in patients with severe ventricular SMR undergoing mitral TEER.4
bPlease refer to Table S2 of the ESC/EACTS Guidelines Supplementary data.4
CAD: coronary artery disease; CRT: cardiac resynchronisation therapy; GDMT: guideline-directed medical therapy; HF: heart failure; HTx: heart transplantation; LVAD: left ventricular assist device; MV: mitral valve; SMR: secondary mitral regurgitation; TEER: transcatheter edge-to-edge repair.
A large proportion of patients with heart failure are affected by SMR, which is associated with worsened prognosis. Timely diagnosis with high-quality imaging and early referral for Heart Team assessment are therefore essential for accurate evaluation and optimal management of these patients.7

In the new guidelines, there are many changes which will affect clinical practice. GDMT should be implemented as fast as possible; one should not wait too long, because the volume load of the ventricle by mitral incompetence is of course deleterious. The heart failure specialist becomes more important and there is such a close interaction between medical treatment and intervention.*
-Professor Michael Böhm, MD Saarland University Hospital, Homburg, Germany
*Expert opinions, advice and all other information expressed represent contributors' views and not necessarily those of Edwards Lifesciences.


I was operated on Thursday and was able to go back home the following Tuesday. I felt really good! I was allowed to start walking again a day later. The shortness of breath was, all of a sudden, gone. My quality of life has increased enormously.
-Reinhold, MR patient
For a listing of indications, contraindications, precautions, warnings, and potential adverse events, please refer to the Instructions for Use (consult eifu.edwards.com where applicable).
PP--EU-10738 v2.0