Step 1
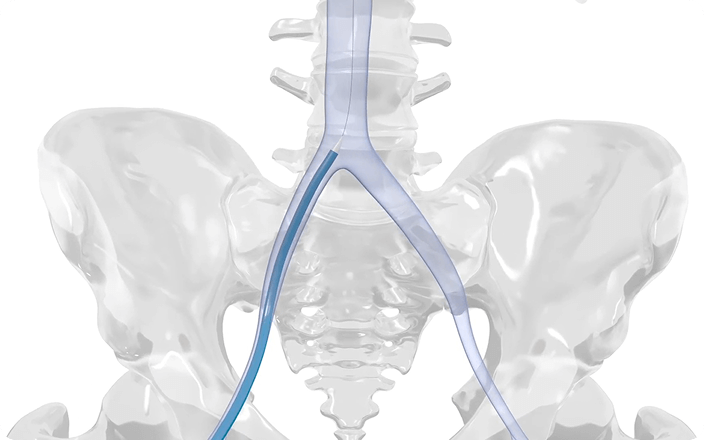
Patient is anaesthetised or sedated. Access is gained to the right femoral vein via a transvenous transfemoral approach.
A growing body of evidence supports TEER for patients with clinically significant, symptomatic mitral regurgitation (MR) who are at high or prohibitive surgical risk – even in those with complex anatomies.1–3
Mitral TEER, also referred to as transcatheter mitral valve repair (TMVr), is a percutaneous catheter-based approach that aims to restore mitral valve leaflet coaptation, thus reducing MR.4
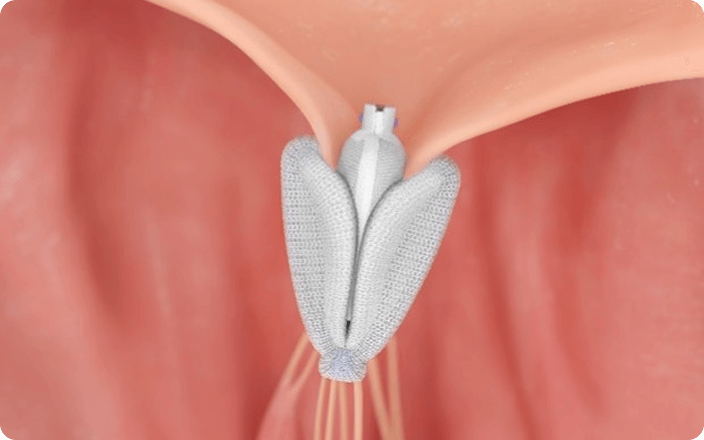
TEER is a minimally invasive technique that approximates the anterior and posterior mitral valve leaflets by grasping them with a clasping device.5
Patient is anaesthetised or sedated. Access is gained to the right femoral vein via a transvenous transfemoral approach.
A guidewire is advanced to the superior vena cava and used to position the transseptal sheath, and a needle is inserted for a conventional percutaneous transseptal puncture.
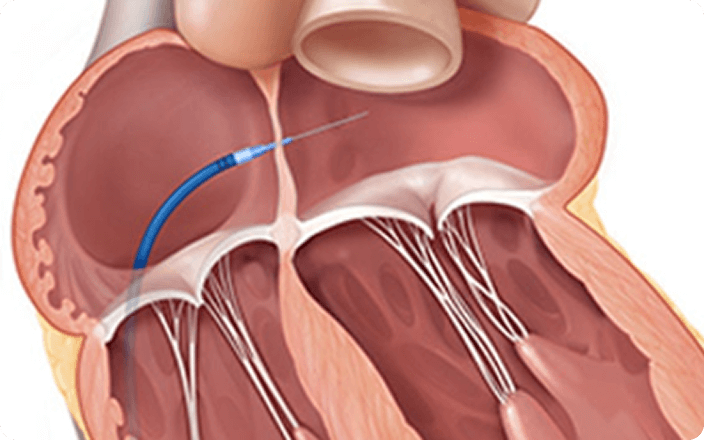
The sheath and needle are advanced to the left atrium. The needle is removed, and a guidewire for the guide catheter is advanced to the left superior pulmonary vein.

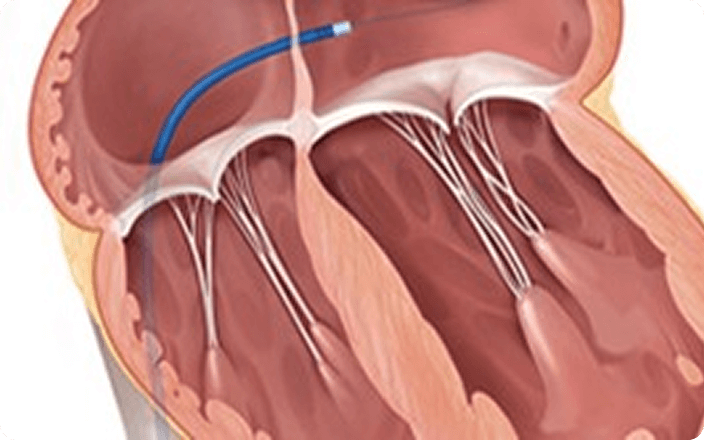
The implant delivery system is advanced through the left atrium to the left ventricle using a guide catheter and introducer.
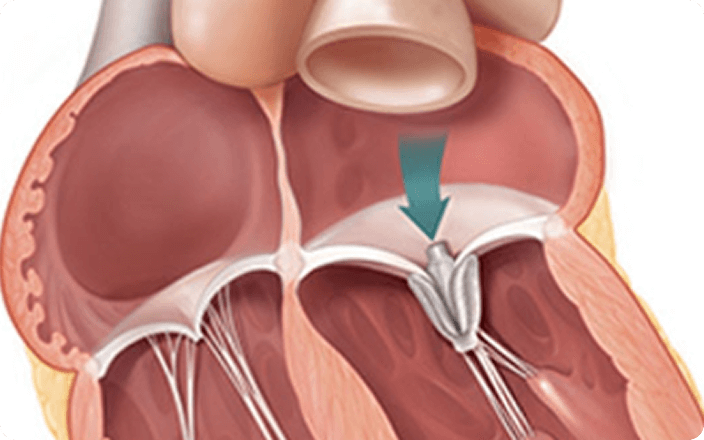
The implant grasps the leaflets, and the residual MR severity and mitral valve gradient are assessed. The implant is repositioned if needed, or another implant is added.
Once the optimal residual MR and gradient are achieved, the implant delivery system is removed, and the access site is closed.

In 2024, 2-year data were released for the MiCLASP study, the CLASP IID trial and the CLASP IID registry.2,3 The findings are very assuring for interventional cardiologists, referring colleagues and for patients, and will hopefully contribute to increased confidence in TMVr in a broad spectrum of MR.*
-Professor Dr med. Tobias Geisler
University Hospital Tübingen, Germany
* Expert opinions, advice and all other information expressed represent contributors' views and not necessarily those of Edwards Lifesciences.
Sustained safety and effectiveness of TEER at 2 years in patients with significant, symptomatic MR in a post-market setting.3


Freedom from CV mortality

Freedom from HFH

NYHA class I/II

KCCQ-OS
*Baseline versus 2 years (n=228; MR ≤1+=80.7%; MR ≤2+=98.3%).
CV: cardiovascular; HFH: heart failure hospitalisation; KCCQ-OS: Kansas City Cardiomyopathy Questionnaire Overall Summary Score; NYHA: New York Heart Association.

The advantage of transcatheter techniques is that they’re minimally invasive. You treat the disease, and it doesn’t involve a long stay in hospital.*
-Dr med. Dabit Arzamendi
Hospital Sant Pau, Barcelona, Spain
* Expert opinions, advice and all other information expressed represent contributors' views and not necessarily those of Edwards Lifesciences.
TEER could be especially beneficial for patients with DMR who have been turned down for surgery due to high risk or other health concerns.6
In the CLASP IID trial, TEER has shown significant and sustained MR reduction in patients with severe, symptomatic DMR at prohibitive surgical risk at 2 years.2


Freedom from CV mortality

Freedom from HFH

NYHA class I/II

KCCQ-OS
*Data from unpaired analysis. The presented MR reduction was achieved using the PASCAL system. CV: cardiovascular; HFH: heart failure hospitalisation; KCCQ-OS: Kansas City Cardiomyopathy Questionnaire Overall Summary Score; MR: mitral regurgitation; NYHA: New York Heart Association.
These 2-year outcomes extend to patients with complex mitral anatomy, who were ineligible for the CLASP IID trial but were enrolled in the CLASP IID registry.2


Freedom from CV mortality

Freedom from HFH

NYHA class I/II

KCCQ-OS
*Data from unpaired analysis.
CV: cardiovascular; HFH: heart failure hospitalisations; KCCQ-OS: Kansas City Cardiomyopathy Questionnaire Overall Summary Score; MR: mitral regurgitation; NYHA: New York Heart Association.
Reduction in all-cause mortality with current therapies for HF range from approximately 15% to 40%, with the highest reduction being reported for TEER treatment.7


*p<0.001
GDMT: guideline-directed medical therapy; KCCQ-OS: Kansas City Cardiomyopathy Questionnaire Overall Summary Score; TEER: transcatheter-edge-to-edge repair.
When I could get back to playing the sports I had given up, it gives me incredible satisfaction.
-Jaume, MR patient

For a listing of indications, contraindications, precautions, warnings, and potential adverse events, please refer to the Instructions for Use (consult eifu.edwards.com where applicable).
PP--EU-10737 V2.0
Edwards Lifesciences Sàrl • Route de l’Etraz 70, 1260 Nyon, Switzerland • edwards.com